Florida HIPAA Compliance: What the Breach Data Shows
In April 2026, healthcare data breaches were reported in 25 US states, the District of Columbia, and Puerto Rico. California logged the most incidents that month, six. Florida logged three, tied with Virginia. Yet Florida’s total individuals affected, 331,316, was the highest of any state in the country that month, ahead of Illinois, Pennsylvania, and every other state on the list.
Nearly all of that figure traces to one source. Florida Physician Specialists, a Jacksonville-based physician practice running eight clinics across three specialty divisions, disclosed a hacking incident affecting 276,498 patients, exposing full names, Social Security numbers, driver’s license numbers, financial account information, and medical and health insurance details. It was the single largest healthcare data breach reported to the HHS Office for Civil Rights (OCR) anywhere in the country that month.
One month earlier, the same publication’s March data showed the pattern reversed: Florida had the second-highest breach count in the US that month, six incidents, but ranked eighth in individuals affected, a fraction of Texas’s 2,831,263. Breach frequency and breach severity moved in opposite directions for the same state two months apart, because a single large incident, not the count of incidents, decides a month’s total.
What decides how large that single incident gets is a separate question, and April’s answer points to a specific failure mode. When OCR settled with four HIPAA-regulated entities in April 2026 over ransomware-related violations, every settlement named the same root cause, a risk analysis failure. The HIPAA Security Rule requires a comprehensive risk analysis and an ongoing risk management program under 45 CFR §164.308, and an accurate risk analysis depends on an accurate inventory of what is actually running on the network.
No healthcare organization can predict whether its next incident will look like Florida’s April or its March, one outlier record or a spread of smaller ones. What it can control is how fast a known vulnerability gets closed on its highest-exposure assets, and that depends on knowing what those assets are, how critical each one is, and what else depends on them. That real-time, accurate map of the estate is what a HIPAA Security Rule risk analysis is supposed to produce, and it is the mechanism that makes ongoing HIPAA compliance defensible under audit.
Florida’s compliance stack runs deeper than HIPAA alone
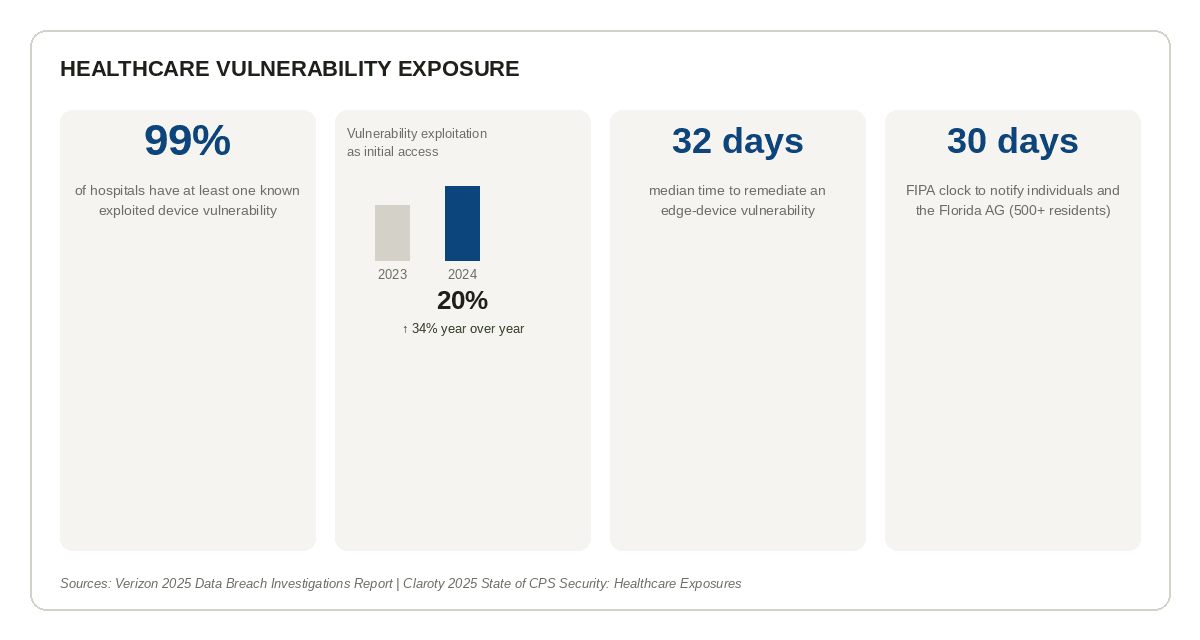
Florida healthcare providers answer to more than the federal Security Rule. The Florida Information Protection Act (FIPA) sets a state notification clock separate from HIPAA’s: 30 days to notify affected individuals from the point a breach is confirmed, extendable to 45 days on a documented showing of good cause, against HIPAA’s federal window of 60 days. Where the two rules diverge, the shorter and more protective deadline controls, which in practice means Florida providers build incident response around the state clock, not the federal one.
A third layer sits on top through the Agency for Health Care Administration (AHCA), which enforces facility-level privacy expectations for licensed Florida providers that don’t map exactly onto HIPAA’s requirements. For the state’s dense network of federally qualified health centers (FQHCs) and rural or critical access hospitals concentrated in the Panhandle, North Central Florida, and the agricultural region south of Lake Okeechobee, a fourth layer applies: HRSA and CMS Conditions of Participation, federal overlays specific to safety-net providers.
None of these regimes conflicts with the others so much as they compound. Each one assumes an organization can answer a basic question quickly: what was touched, and how many people does it affect. FIPA’s 30-day clock only works if scoping doesn’t take 30 days on its own. That assumption is where the gap actually shows up.
Where the four-month scoping window comes from
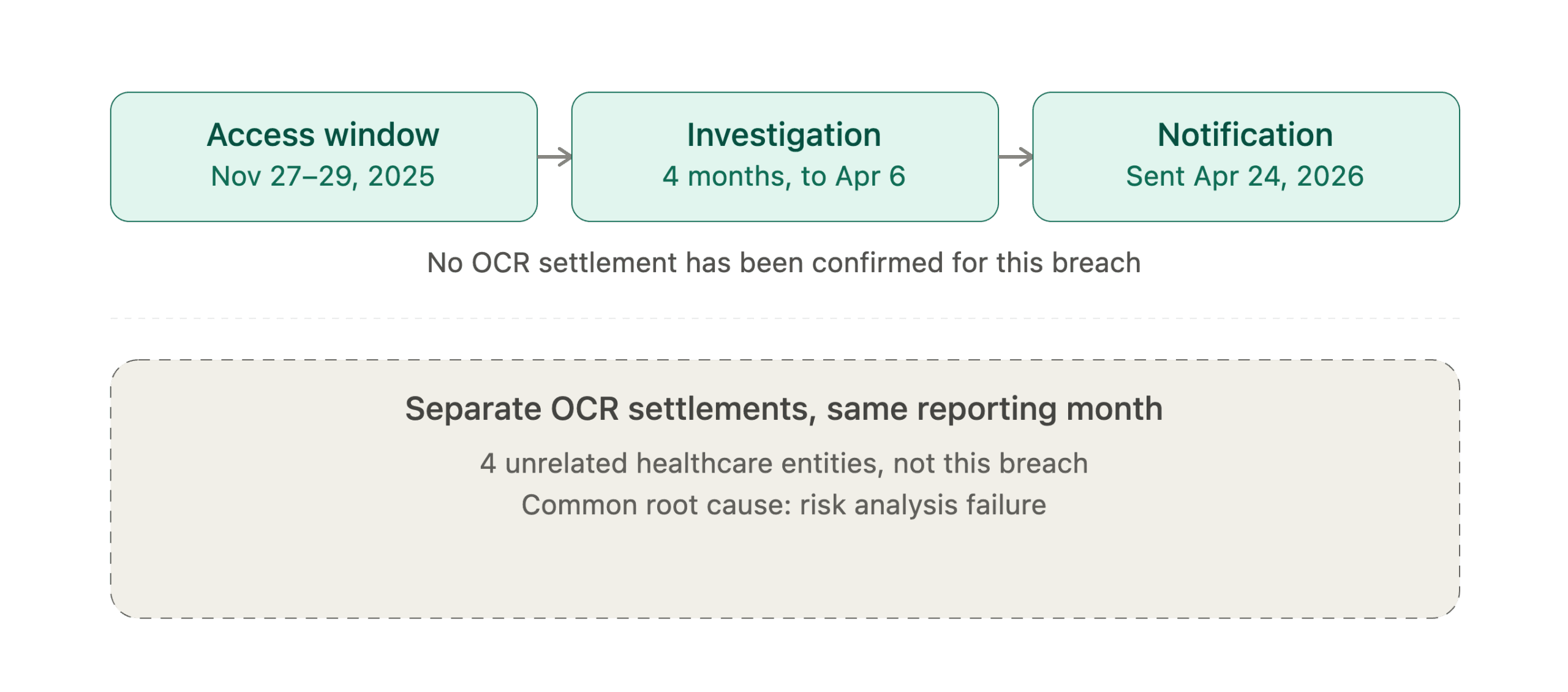
Florida Physician Specialists’ own disclosure lays out a specific timeline. Unauthorized access to its network occurred over a two-day window, November 27 to November 29, 2025. The investigation into what had been touched concluded on April 6, 2026, more than four months later. Individual notification began April 24, 2026, another eighteen days after that.
The practice has not disclosed how the attacker gained access, whether a vulnerability was exploited, or whether ransomware was involved, and no ransomware group has claimed responsibility. That detail may never become public. What the timeline does show, independent of cause, is the shape of the gap: a two-day access window took over four months to scope. An intrusion that short doesn’t require four months to characterize if the systems it touched are already mapped, catalogued, and bounded. It does if scoping means reconstructing, after the fact, what was connected to what.
That reconstruction problem is the same one showing up across OCR’s enforcement docket. Every one of the four HIPAA settlements OCR announced in April 2026, covering a healthcare provider, a business associate, and a health plan, cited a risk analysis failure as a violation. It remains the most commonly identified Security Rule violation in OCR’s enforcement history. A risk analysis is only as accurate as the asset inventory feeding it, and an inventory built after an incident, under pressure, on a state notification clock, is a different exercise than one maintained continuously beforehand.
Severity is unpredictable, and the data says why
Florida’s April-to-March reversal isn’t an isolated fluke of one state’s reporting cycle. It reflects a broader pattern in how healthcare breaches actually happen.
Vulnerability exploitation has grown into a larger share of how attackers get in. Verizon’s 2025 Data Breach Investigations Report found vulnerability exploitation accounted for 20% of initial access vectors, up 34% year over year. Across the same data, only about 54% of edge-device vulnerabilities were fully remediated within the year they were disclosed, with a median remediation time of 32 days.
The scale of the exposure compounds the timing problem. Claroty’s 2025 analysis of 2.25 million connected medical devices across 351 healthcare organizations found known, exploited vulnerabilities present in 99% of hospitals and health delivery organizations studied.
Sophos’s 2025 healthcare-sector survey found exploited vulnerabilities became the leading technical root cause of ransomware attacks on healthcare providers that year, used in 33% of incidents, the first time in three years vulnerabilities topped the list for the sector.
Put together, these numbers describe an industry where known vulnerabilities are common, remediation is slow, and which vulnerability gets weaponized first is largely outside any one organization’s control. Florida Physician Specialists could have been a 5,000-record incident or a 276,498-record one depending on which system an attacker happened to reach first, and no amount of planning changes that a system will eventually be reached. What planning changes is how much sits exposed on the other side of that first foothold, and how fast the highest-value pieces get closed off once a vulnerability is known.
What an accurate asset map actually does
The lever available to every healthcare provider, regardless of size or budget, is prioritization: knowing which systems hold protected health information, which of those systems are internet-facing or otherwise reachable, and which vulnerabilities on those systems represent the greatest risk if left unpatched.
That prioritization runs on three inputs working together, not one. A CVSS score tells you how severe a vulnerability is in isolation. Asset criticality tells you how important the affected system is to the organization. Service dependency mapping tells you what else connects to that system, so a vulnerability on a legacy backup server that feeds an active EMR gets treated differently than the identical vulnerability on an isolated test environment. A configuration management database (CMDB) exists to keep that dependency map current as the estate changes, servers get decommissioned, new devices get provisioned, integrations get added, so that risk analysis and vulnerability response are working from what’s actually running today rather than what was documented at the last audit cycle.
Virima’s ViVID service maps supply that third input specifically. They don’t detect vulnerabilities on their own; a vulnerability scanner still generates the CVSS scores. What ViVID adds is the connective layer: showing which services and assets a given vulnerability actually touches, so a patching team facing a backlog of known issues can close the ones with the widest blast radius first, instead of working through a flat list ordered by severity score alone. For a healthcare estate spread across billing systems, EMR interfaces, imaging archives, and a long tail of legacy servers, that dependency context is often the difference between a scoping review that takes days and one that takes months.
The variable that stays in an organization’s control
For Florida providers, that lever matters against a compressed timeline most other states don’t share. FIPA’s 30-day notification clock and HIPAA’s risk-analysis requirement both assume an organization can answer “what was touched” fast. An estate mapped continuously, not reconstructed after the fact, is what makes that answer possible inside 30 days instead of four months.
For Florida providers building compliance programs against HIPAA’s Security Rule requirements alongside FIPA, AHCA, and HRSA/CMS obligations, that answer is worth getting right before it’s needed under a 30-day clock. An estate that’s mapped continuously, not reconstructed after the fact, is the difference between a risk analysis that holds up under OCR review and one that gets flagged as the fifth version of the same violation.
Schedule a demo to see how Virima supports continuous asset mapping for Florida HIPAA compliance →